Hair thinning is one of the most clinically mismanaged conditions in Malaysian dermatology — not because treatments don't exist, but because the wrong treatment is applied to the wrong type. A patient with telogen effluvium receiving DHT-blocking therapy will see no improvement. A patient with androgenetic alopecia given iron supplements will lose six months of the critical intervention window. Correct diagnosis is the treatment.
This guide presents a systematic framework for identifying the biological subtype of your hair thinning. Each type has a distinct mechanism, a distinct distribution pattern, and requires a distinct clinical response. Work through the diagnostic decision tree below before committing to any treatment protocol.
The Diagnostic Decision Tree
The first clinical signal is *where* on the scalp the thinning originates. Pattern and location narrow the probable diagnosis before any laboratory work.
| Location of Thinning | Likely Cause | Confirm With | |---|---|---| | Crown + temples, gradual | Androgenetic alopecia (DHT-mediated) | Trichoscopy: miniaturised follicles, varied shaft diameter | | Diffuse, whole scalp | Telogen effluvium (acute stress, illness, diet) | Hair pull test; serum ferritin, TSH, CRP | | Frontal hairline recession | Traction alopecia or frontal fibrosing alopecia | History of tight hairstyles; trichoscopy for perifollicular fibrosis | | Patchy, circular bald spots | Alopecia areata (autoimmune) | Exclamation-mark hairs at patch margin; ANA panel | | Diffuse postpartum (3–6 months) | Postpartum telogen effluvium | Delivery timing; serum ferritin, thyroid panel | | Diffuse with fatigue, pallor | Iron deficiency or thyroid dysregulation | Serum ferritin (<30 µg/L), free T4, TSH | | Hairline + temples, history of tight styling | Traction alopecia | Hairstyle history; trichoscopy for cast formation | | Diffuse with scaling, itch, erythema | Scalp inflammation (seborrheic dermatitis, psoriasis) | Clinical examination; dermoscopy |
The 8 Clinical Subtypes
1. Telogen Effluvium The most common cause of sudden diffuse shedding in Malaysian women. A physiological shock — surgery, fever, dengue recovery, crash dieting, or severe psychological stress — pushes a disproportionate number of follicles into the resting (telogen) phase simultaneously. Shedding peaks 2–4 months after the trigger event. The scalp itself is healthy; follicles are intact. Most cases resolve within 6 months once the trigger is removed. Chronic telogen effluvium, lasting beyond 6 months, requires deeper systemic investigation per Whiting (1996).
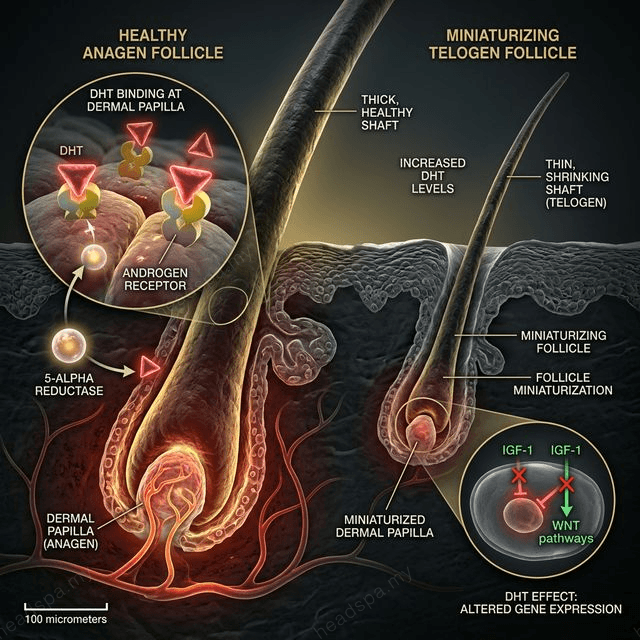
2. Androgenetic Alopecia Driven by DHT (dihydrotestosterone) binding to androgen receptors in susceptible follicles, causing progressive miniaturisation. In men: Hamilton-Norwood pattern (temples and crown). In women: Ludwig pattern (crown widening, preserved frontal hairline). Trichoscopy is essential — early-stage androgenetic alopecia cannot be distinguished from chronic telogen effluvium by visual inspection alone. Miniaturised hairs (shaft diameter <0.03 mm) and diameter variability >20% confirm the diagnosis. See [/concerns/hair-fall](/concerns/hair-fall) for detailed follicle anatomy.
3. Alopecia Areata An autoimmune attack on the hair follicle, mediated by CD8+ T-cells targeting follicular melanocytes. Presents as sharply demarcated circular patches with smooth scalp skin and "exclamation-mark" hairs at the patch periphery — a pathognomonic sign. It can progress to alopecia totalis (entire scalp) or universalis (entire body). Treatment requires immune modulation, not scalp-based therapies alone. For the full clinical pathway, see [/blog/alopecia-areata-treatment-malaysia](/blog/alopecia-areata-treatment-malaysia).
4. Postpartum Hair Loss A physiological subtype of telogen effluvium, hormonally synchronised. Elevated oestrogen during pregnancy prolongs the anagen (growth) phase, retaining hairs that would normally shed. Post-delivery, oestrogen withdrawal triggers synchronised telogen conversion, producing dramatic shedding at 3–6 months postpartum. Follicles are not damaged; spontaneous recovery is expected by 12 months. Iron stores are frequently depleted during pregnancy and must be assessed concurrently. See [/blog/postpartum-hair-loss-malaysia](/blog/postpartum-hair-loss-malaysia).
5. Iron Deficiency Ferritin — the storage form of iron — is the critical marker, not haemoglobin. A patient can be non-anaemic with severely depleted ferritin stores insufficient for follicle matrix cell division. The threshold most associated with hair loss is ferritin <30 µg/L. Malaysian dietary patterns with low red meat intake and heavy tea consumption (tannins inhibit iron absorption) create structural risk. See [/blog/iron-deficiency-hair-loss-malaysia](/blog/iron-deficiency-hair-loss-malaysia).
6. Thyroid Dysregulation Both hypothyroidism and hyperthyroidism produce diffuse telogen effluvium. Thyroid hormone receptors are expressed on follicular keratinocytes; disruption impairs the anagen-to-catagen transition. TSH elevation alone does not always produce hair loss — free T4 levels are the more sensitive marker. Subclinical hypothyroidism is significantly underdiagnosed in Malaysian women of reproductive age.
7. Traction Alopecia Caused by repeated mechanical tension on the follicle root — tight inner caps, safety pins at the hairline, pulled-back ponytails worn chronically. Early stages are reversible; late-stage follicular fibrosis is not. Malaysian Muslim women face disproportionate risk due to specific hijab styling practices. See [/blog/traction-alopecia-hijab-malaysia](/blog/traction-alopecia-hijab-malaysia) for the full follicle damage model.
8. Scalp Inflammation Seborrheic dermatitis, psoriasis, and contact dermatitis produce a hostile follicular microenvironment — elevated IL-17, IL-22, and TNF-α drive premature catagen and inhibit anagen re-entry. Chronic scalp inflammation is an underrecognised driver of diffuse hair thinning. Treatment of the underlying dermatosis frequently reverses the hair loss. See [/blog/androgenetic-alopecia-men-malaysia](/blog/androgenetic-alopecia-men-malaysia) for the interaction between DHT and scalp inflammation.
When Trichoscopy Is Essential
Trichoscopy — dermoscopic examination of the scalp at ×10–×70 magnification — is not optional when visual assessment yields ambiguity. The following clinical scenarios require trichoscopy to avoid misdiagnosis:
- Distinguishing androgenetic alopecia from chronic telogen effluvium (both present as diffuse thinning)
- Identifying perifollicular fibrosis in early traction alopecia before it becomes irreversible
- Confirming alopecia areata in early-stage patches with insufficient exclamation-mark hairs
- Detecting yellow dots (sebaceous plugging) in androgenetic alopecia vs empty follicles in scarring alopecias
TTE Elephant's trichoscopy assessment maps follicle density, shaft diameter variability, and perifollicular inflammation in a single session. Book at [/headspa-kl](/headspa-kl) (Kuala Lumpur) or [/headspa-jb](/headspa-jb) (Johor Bahru).
FAQ
Q: My hair is thinning all over — does that mean it's definitely telogen effluvium? A: Diffuse thinning is consistent with telogen effluvium, but also with chronic telogen effluvium, female-pattern androgenetic alopecia, iron deficiency, and thyroid dysregulation. A hair pull test and baseline bloods (ferritin, TSH, free T4, CBC) are the minimum workup. Trichoscopy adds follicular-level data that bloodwork cannot provide.
Q: Can I have two types of hair thinning simultaneously? A: Yes. The most common combination is androgenetic alopecia compounded by telogen effluvium — the underlying miniaturisation becomes clinically visible during an effluvium episode. This is why some patients experience sudden worsening after stress or illness, which then only partially recovers.
Q: How long does it take to confirm a diagnosis? A: Trichoscopy provides structural data in a single session. Laboratory panels take 3–5 business days. A provisional clinical diagnosis is usually established within one week. Treatment response monitoring — the final confirmation — takes 3–6 months.
Q: Is hair thinning at the temples always androgenetic alopecia? A: Not always. Traction alopecia from tight hairstyles and frontal fibrosing alopecia both target the temporal and frontal hairline. The distinguishing feature is perifollicular fibrosis on trichoscopy, which is absent in androgenetic alopecia. Hairstyle history is a critical part of the clinical interview.
Q: At what point is hair thinning no longer reversible? A: Once a follicle is replaced by fibrous tissue — scarring alopecia — regrowth from that follicle is not possible with current therapies. This threshold is why early trichoscopy is clinically important: identifying fibrosis before the follicle is fully replaced preserves the intervention window.
