
Losing 50–100 hairs per day is not a problem. It is the normal completion of the hair growth cycle, repeated continuously across 100,000 follicles. The clinical distinction between hair fall and hair loss is one of mechanism, not volume alone — and conflating the two leads to inappropriate treatment choices and measurable delays in effective intervention.
What Hair Fall Is 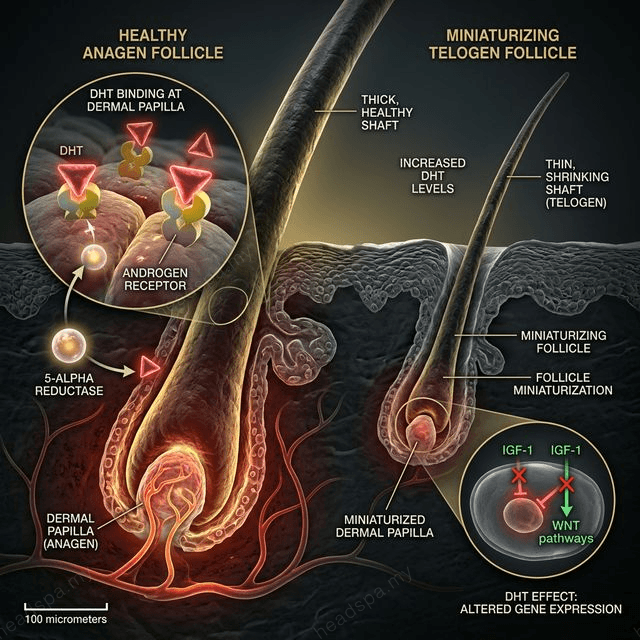
Hair fall refers to the natural shedding that occurs at the end of the telogen (resting) phase of the hair growth cycle. Each follicle cycles independently through three phases: anagen (growth, 2–7 years), catagen (regression, 2–3 weeks), and telogen (resting and shedding, 3–4 months). At any given time, approximately 10–15% of follicles are in telogen — shedding their hair fibre and preparing for the next anagen cycle.
Normal daily hair fall produces hairs with a visible white bulb at the root — the fully keratinised telogen club hair. These hairs have completed their cycle. The follicle is intact and will regenerate. This is not a pathological event.
What Hair Loss Is
Hair loss is a condition in which follicles fail to regenerate — either because they are damaged, miniaturised, or permanently destroyed. The critical distinction: in hair loss, the follicle is the problem. In hair fall, the follicle is functioning normally.
The principal categories of true hair loss are:
Androgenetic alopecia (AGA): DHT (dihydrotestosterone) binds to androgen receptors in genetically susceptible follicles, progressively shortening the anagen phase with each cycle. The follicle miniaturises over years — producing progressively finer, shorter hairs until it becomes vellus (non-pigmented, near-invisible) and eventually dormant. This is permanent if untreated. It accounts for approximately 95% of male pattern baldness and 40% of female diffuse thinning.
Alopecia areata: An autoimmune condition in which T-lymphocytes attack follicle cells in anagen phase. Presents as discrete circular bald patches. The follicle is not destroyed — it is suppressed. Spontaneous recovery occurs in 50% of cases within 1 year. Immunological intervention is required for persistent cases.
Scarring alopecia: Follicle destruction through fibrosis — the follicle unit is replaced by scar tissue. Causes include untreated folliculitis, traction alopecia progressed to fibrosis, and certain autoimmune conditions (lichen planopilaris, discoid lupus). This is permanently irreversible at the affected sites.
The Diagnostic Middle Ground: Telogen Effluvium
Telogen effluvium occupies the space between normal hair fall and true hair loss. A triggering event — acute illness, surgery, postpartum hormonal shift, severe psychological stress, or nutritional deficiency — abruptly shifts a large proportion of anagen follicles into early telogen simultaneously. Two to four months later, those follicles shed their hairs together, producing what feels like alarming diffuse hair fall.
The follicles are structurally intact. This is accelerated hair fall, not hair loss — the distinction is the difference between a reversible event and a permanent one. Without a triggering cause resolved, however, telogen effluvium can become chronic (persisting beyond 6 months), and chronic cortisol elevation can push the condition toward early androgenetic progression.
How to Tell the Difference
White-bulb hairs in the shower: Normal telogen shedding. The follicle is intact.
Diffuse thinning with shortened hair cycle (hair feels thinner each regrowth): AGA pattern. Requires DHT-blocking intervention and cycle length support.
Circular bald patches with sharp margins: Alopecia areata. Requires dermatologist assessment.
Sudden diffuse shedding 2–4 months after a major stressor: Telogen effluvium. Reversible if the stressor is resolved.
Trichoscopy — the same AI-assisted scalp imaging used at TTE Elephant before every session — distinguishes these patterns definitively within a 15-minute scan. Follicle miniaturisation (AGA), empty follicle units (scarring), and uniform telogen density (effluvium) are visually distinct under magnification. Self-diagnosis based on volume alone is unreliable. Diagnosis precedes treatment — in every case.
