A Malaysian woman sees her doctor for hair loss. Her full blood count returns with haemoglobin at 12.1 g/dL — technically within the normal female reference range. Her doctor tells her her iron is fine. She leaves without a ferritin result.
Three months later, her hair fall has not improved. She purchases a scalp serum. She changes her shampoo. The shedding continues.
Her ferritin, had it been tested, would likely read between 10 and 25 µg/L. The research-validated threshold for optimal hair follicle function is 70 µg/L. The gap between her actual level and what her follicles require explains exactly why her hair is still falling — and why no topical product will resolve it.
Iron deficiency without anaemia is the most systematically underdiagnosed cause of diffuse hair loss in Malaysian women. Understanding why requires understanding the difference between serum iron, haemoglobin, and ferritin.
Why Ferritin Is the Correct Metric
Serum iron measures the amount of iron currently circulating in your blood — a value that fluctuates hour-to-hour based on recent dietary intake and is not a reliable indicator of iron stores. Haemoglobin measures the red blood cell protein that carries oxygen — it only drops below range when iron depletion has progressed to the point of full anaemia.
Ferritin is the storage protein that holds iron in reserve — primarily in the liver, spleen, and bone marrow. It is the earliest indicator of iron depletion, falling long before serum iron or haemoglobin become abnormal. A ferritin of 12 µg/L with normal haemoglobin means the body has nearly exhausted its iron reserves but has not yet entered clinical anaemia.
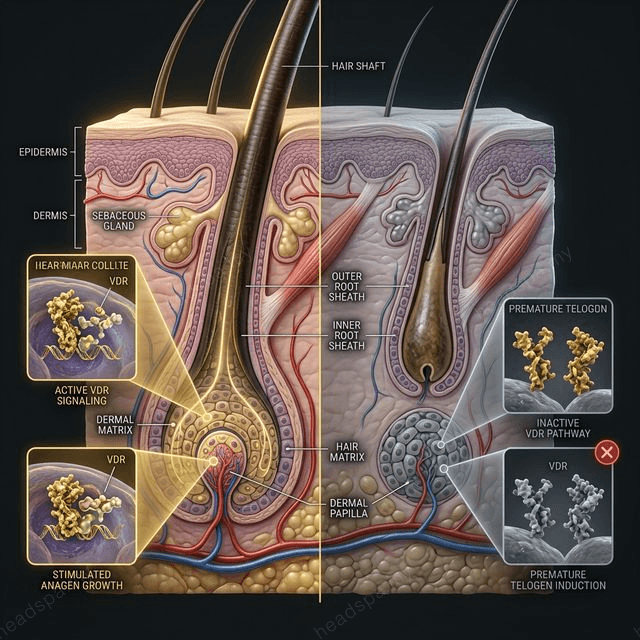
The hair follicle does not wait for anaemia to be affected by iron status. The follicle matrix — the most rapidly dividing cell population in the human body — is disproportionately sensitive to iron availability because iron is a required cofactor for ribonucleotide reductase, the rate-limiting enzyme in DNA synthesis. When iron stores fall below functional threshold, follicle mitosis slows. The anagen phase shortens. More follicles enter telogen simultaneously. Diffuse shedding follows.
The Ferritin Thresholds That Matter
Laboratory reference ranges for ferritin (typically 12–150 µg/L for women) are calibrated to identify iron deficiency anaemia — not to optimise hair follicle function. The gap between "not anaemic" and "enough iron for hair growth" is clinically significant.
| Ferritin Level | Clinical Interpretation | Hair Follicle Impact | |---|---|---| | < 12 µg/L | Iron deficiency (frank depletion) | Severe impairment; systemic symptoms likely | | 12–30 µg/L | Depleted stores; non-anaemic | Significant hair loss; follicle mitosis compromised | | 30–50 µg/L | Sub-optimal; borderline | Mild-to-moderate shedding; follicle recovery impaired | | 50–70 µg/L | Low-normal; inadequate for hair | Latent shedding; slow anagen re-entry | | > 70 µg/L | Adequate for follicle function | Optimal hair growth supported | | > 100 µg/L | Optimal recovery range | Recommended target for active hair loss treatment |
The 70 µg/L threshold for hair follicle optimisation was established by Rushton (2002) and subsequently supported by Trost et al. (2006). It is not fringe science — it is the standard cited in dermatology hair loss guidelines, but it rarely reaches the primary care consultation.
Why Malaysian Women Are Disproportionately Affected
The Malaysian dietary and physiological context creates a perfect confluence of risk factors for low ferritin.
Dietary iron profile: The Malaysian diet is heavily rice-based. White rice contains phytic acid (phytate), an anti-nutrient that binds non-haem iron and reduces its intestinal absorption by up to 80%. A meal of nasi lemak or nasi putih with leafy vegetables provides theoretical iron content — but the bioavailable fraction reaching the bloodstream is a fraction of the label value.
Teh tarik, teh O, and coffee — consumed with or immediately after meals as is common in Malaysian food culture — contain tannins that further inhibit non-haem iron absorption. A woman who drinks two cups of tea with her meals reduces iron absorption from those meals by approximately 60% per cup.
Menstruation: Heavy menstruation (menorrhagia), defined as blood loss exceeding 80 mL per cycle, is more prevalent than clinically recognised. Each mL of menstrual blood contains approximately 0.5 mg of elemental iron. Women with heavy periods may lose 40–60 mg of iron per cycle — an amount that rice-based, low-red-meat diets cannot reliably replenish.
Vegetarian and semi-vegetarian dietary patterns: Across Indian Malaysian and certain Chinese Malaysian communities, low or absent red meat consumption reduces haem iron intake significantly. Haem iron (from animal sources) is absorbed at 15–35% efficiency; non-haem iron (from plant sources) is absorbed at 2–20% depending on meal composition. The gap is material.
Postpartum depletion: As detailed in our [postpartum hair loss guide](/concerns/postpartum-hair-loss), pregnancy and breastfeeding create compound iron depletion that often goes uncorrected between pregnancies. Women who lose hair both postpartum and between pregnancies are frequently in a state of chronic ferritin depletion.
Iron-Rich Malaysian Foods: A Clinical Perspective
| Food | Serving | Iron (mg) | Type | Notes | |---|---|---|---|---| | Beef liver (hati lembu) | 100g | 6.5 mg | Haem | Highest bioavailable source | | Clams / lala | 100g | 3.0 mg | Haem | Common in KL / JB hawker menus | | Tempeh | 100g | 2.7 mg | Non-haem | Fermentation reduces phytate; improves absorption | | Kangkung (water spinach) | 1 cup cooked | 2.5 mg | Non-haem | Pair with vitamin C, not tea | | Bayam (spinach) | 1 cup cooked | 2.1 mg | Non-haem | Oxalates limit absorption | | Edamame / soybeans | 100g | 2.0 mg | Non-haem | Phytate present; eat with acidic foods | | Dried apricots | 50g | 1.7 mg | Non-haem | Practical snack option | | Fortified cereals | 30g serving | 4.0–8.0 mg | Non-haem | Varies by brand; check labels |
To enhance non-haem iron absorption: consume iron-rich foods with vitamin C (e.g., a squeeze of lime, or a small glass of orange juice); avoid teas and coffee for 60 minutes before and after iron-containing meals; separate calcium-rich foods (dairy) from iron-rich meals by at least two hours.
The TTE Elephant Clinical Protocol
At TTE Elephant, all consultations for diffuse hair loss begin with a structured intake assessment that screens for iron deficiency risk factors before any scalp treatment is recommended. If the clinical picture is consistent with nutritional telogen effluvium — diffuse shedding, no visible scalp inflammation, normal follicle density at trichoscopy but reduced anagen-to-telogen ratio — we provide a written referral recommendation for ferritin testing (not serum iron alone) from the patient's physician or lab.
This is not a sales strategy. It is the correct clinical sequence: identify the root cause, address it systemically, and use scalp treatment to support the follicle microenvironment during recovery. Treating a ferritin-depleted scalp with topical serums without addressing the nutritional deficit produces no meaningful outcome.
Our [hair fall assessment](/concerns/hair-fall) includes trichoscopy-guided follicle density measurement that provides baseline data before and after nutritional correction, enabling patients to track actual follicle recovery rather than estimating from hair counts alone.
Scalp circulation protocols at our [KL](/headspa-kl) and [JB](/headspa-jb) locations support micronutrient delivery to the follicle bulb — a meaningful adjunct once ferritin is being corrected, because improved blood flow ensures that the iron being replenished reaches the follicle matrix efficiently.
---
Q: My doctor said my blood test is normal. Why does my hair keep falling? A: Standard blood panels typically include haemoglobin and serum iron — metrics calibrated for anaemia detection, not hair follicle function. If your ferritin was not specifically tested, you do not have a complete picture of your iron status. Request a serum ferritin test explicitly, and assess the result against the 70 µg/L threshold for optimal hair follicle support — not just the laboratory reference range.
Q: How long does it take for hair to recover after ferritin is corrected? A: Ferritin repletion to optimal levels typically takes three to six months of consistent supplementation. Hair follicle response lags behind ferritin normalisation by an additional two to three months, because follicles that entered telogen due to iron depletion must complete the resting phase before re-entering anagen. Total visible improvement timeline: six to nine months from the point of sustained ferritin correction.
Q: Can I get enough iron from food alone, or do I need supplements? A: For women with ferritin below 30 µg/L, dietary modification alone is rarely sufficient to reach and sustain the 70 µg/L threshold — particularly given the absorption-reducing factors in a typical Malaysian diet. Supplementation with elemental iron (ferrous sulphate or ferrous bisglycinate) is typically required for clinical correction. Ferrous bisglycinate is better tolerated with fewer gastrointestinal side effects. Supplement with vitamin C; avoid calcium within two hours of dosing.
Q: Is iron deficiency hair loss different from other types of hair loss? A: Yes, clinically. Iron deficiency produces diffuse telogen effluvium — generalised thinning across the entire scalp with an increased shed count, not patchy loss. It is distinguishable from androgenetic alopecia (which follows a patterned recession) and alopecia areata (which produces discrete circular patches). Trichoscopy at TTE Elephant can characterise the pattern and guide whether nutritional, hormonal, or autoimmune workup is the priority. See our full [hair fall guide](/concerns/hair-fall) for the differential framework.
