Finding painful, red, pimple-like bumps on your scalp can be alarming, but in Malaysia's aggressive tropical climate, it is a highly common dermatological presentation. Colloquially referred to as "scalp acne" or "jerawat kulit kepala," this condition is clinically known as Scalp Folliculitis—an inflammation or infection of the hair follicle.
Treating this condition simply by scrubbing harder with a supermarket anti-dandruff shampoo is often disastrous. Folliculitis is not a single disease entity; it is a spectrum ranging from superficial microbial imbalance to deep, scarring bacterial necrosis. To resolve it permanently, you must first accurately diagnose whether the invading pathogen is bacterial or fungal, and critically address the environmental incubator that allowed it to proliferate.
Why is Scalp Folliculitis So Prevalent in Malaysia?
The human scalp possesses an average of 100,000 hair follicles. Each individual follicle consists of an ostium (the opening on the skin surface), a sebaceous gland, and an intricate mucosal lining. In a healthy state, the scalp’s acidic mantle (pH 4.5–5.5) keeps opportunistic skin flora firmly restricted to the superficial layers.
However, Malaysia's environmental reality systematically dismantles this defense mechanism.
With an average ambient temperature of 32–34°C, scalp sebum viscosity is profoundly reduced. The heat liquefies the protective wax esters, causing them to spread rapidly into the follicular canal. Simultaneously, the 80–90% relative humidity triggers constant, unavoidable micro-sweating. When massive amounts of liquefied sebum mix with trapped sweat, it radically dilutes the crucial acidic mantle. The scalp pH drifts from an antimicrobial 4.5 up to a highly vulnerable 6.5 or 7.0.
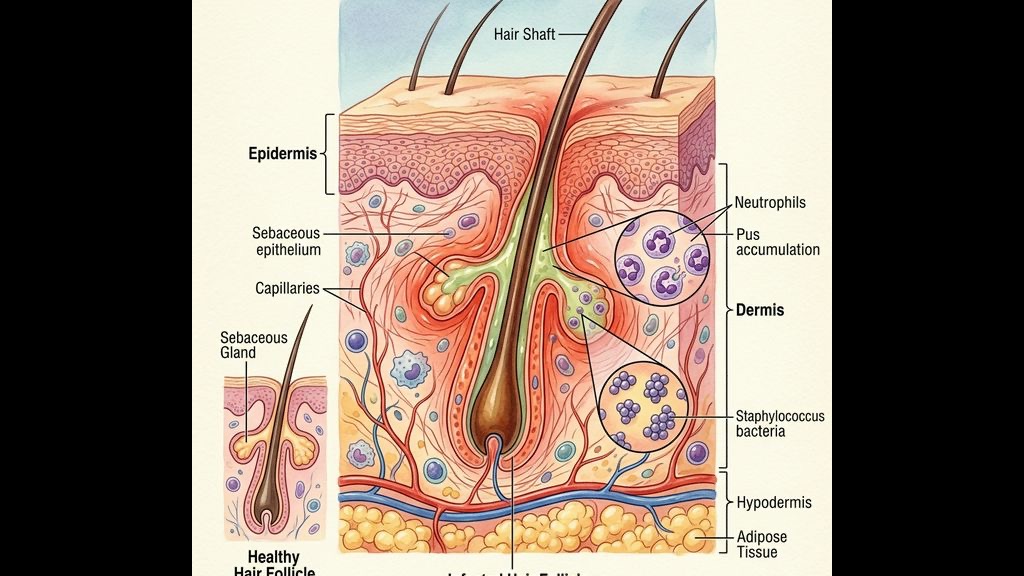
This alkaline, wet, and overheated environment is the absolute perfect biological incubator for rapid microbial colonization. When pathogenic microbes penetrate the compromised barrier and enter the deeper follicular canal, the immune system responds by sending white blood cells (neutrophils) to attack the invader. This massive accumulation of dead bacteria, white blood cells, and oxidized fat is what forms the painful, pus-filled head (pustule) characteristic of folliculitis.
How Does Hijab Occlusion Accelerate the Infection?
This environmental incubator effect is magnified exponentially for Muslimah women. Wearing an inner cap (anak tudung) followed by a hijab physically traps heat and completely abolishes airflow.
As discussed deeply in our [Hijabi Scalp Care](/concerns/hijabi-scalp-care) overview, the microclimate directly under a hijab is frequently 2–4°C hotter than ambient temperature, with humidity trapped at near 100% RH for 8 to 12 hours a day.
Furthermore, the physical tension of the inner cap directly rubbing against the scalp introduces an element of mechanical trauma (friction). Friction chemically weakens the stratum corneum and mechanically forces surface bacteria deeper down into the follicle ostia. This combination—a highly compromised alkaline barrier, massive microbial overgrowth fuel, and mechanical penetration—is why hijab-wearing individuals in tropical urban centers frequently present with chronic, highly recurrent superficial folliculitis primarily concentrated around the hairline and the crown, where friction and sweat pooling are highest.
What is the Clinical Difference Between Bacterial and Fungal Folliculitis?
Because the treatment pathway is entirely different, differentiating the causative pathogen is the absolute most critical step. Relying on visual inspection in the mirror is insufficient. The two predominant culprits acting on the Malaysian scalp are *Staphylococcus aureus* (Bacterial) and *Malassezia* (Fungal).
- Presentation: Bacterial folliculitis typically presents as distinctly isolated, highly inflamed, bright red papules (bumps) that rapidly develop a clear, tense, central pustule (yellow/white pus head) pierced directly by a single hair shaft.
- Symptoms: It is usually acutely tender to the touch (painful rather than intensely itchy) and tends to spread if the pus is ruptured and smeared across adjacent healthy follicles.
- Presentation: *Malassezia* folliculitis typically presents as a widespread, homogenous "crop" of hundreds of very tiny, uniform (monomorphic), extremely itchy, flesh-colored or slightly red papules. They rarely develop massive, tense white pus heads like bacterial infections.
- Symptoms: The hallmark symptom is intense, maddening pruritus (itching), particularly when sweating during exercise or when entering a hot, humid environment like the KL LRT station during rush hour.
Treating Fungal Folliculitis with aggressively prescribed oral antibiotics (designed for bacteria) is a catastrophic medical error, as the antibiotic obliterates competing healthy bacteria, leaving the *Malassezia* an empty ecological niche to overgrow even more aggressively, creating a severe rebound infection.
Why is Trichoscopy Required for Diagnosis?
Because *Staph* and *Malassezia* can occasionally present with overlapping symptoms, or exist concurrently as a polymicrobial infection, naked-eye diagnosis is a massive clinical risk.
At TTE Elephant Head Spa, high-magnification Trichoscopy (60x–200x) is the mandatory first step. Trichoscopically, bacterial folliculitis will show prominent perifollicular erythema (intense redness localized strictly around the follicular opening) with distinct yellow crusting. Conversely, *Malassezia* folliculitis often reveals significant underlying epidermal scaling (dandruff) between the follicles, twisted or coiled intra-follicular hairs struggling to exit the clogged ostia, and a distinct lack of deep, structural scarring.
This visual confirmation dictates the exact intervention pathway—whether we must deploy clinical fungistatic agents or strictly manage the bacterial load.
The TTE Clinical Head Spa vs. The Dermatologist
[Scalp Folliculitis](/concerns/scalp-folliculitis) exists on a spectrum of severity. Transparency regarding clinical limitations is crucial for patient safety.
- The pustules are rapidly enlarging into deep, painful, hard nodules or boils (furuncles/carbuncles).
- You are experiencing systemic signs of infection (fever, swollen lymph nodes in the neck or behind the ears).
- The infection is tracking deep into the dermis, permanently destroying the hair follicle and leaving smooth, hairless, scarred tissue (Folliculitis Decalvans). A head spa *cannot* reverse scarring alopecia. This requires immediate systemic antibiotics (like clindamycin or rifampicin) and potent topical corticosteroids from a licensed physician.
- Your condition is diagnosed as superficial *Malassezia* folliculitis, requiring the massive, hardened layers of oxidized sebum (the fungal food source) to be carefully decalcified from deep within the follicle without using harsh alkaline shampoos that destroy the barrier.
- You suffer from recurrent, mild bacterial folliculitis driven fundamentally by environmental occlusion (like a hijab), requiring a total reset of your scalp's acidic mantle to naturally prevent future bacterial colonization.
- You are currently under dermatological care, but the prescribed medical drying lotions contain high concentrations of isopropyl alcohol that are severely dehydrating your scalp, requiring targeted, non-comedogenic biometric lipid repair to halt the compensatory sebum rebound loop.
TTE’s Preventative Protocol: Restoring the Acidic Shield
Treating a breakout is easy; preventing its immediate return requires altering the biological environment.
Our clinical protocol focuses entirely on barrier restoration. We begin by dissolving the deep-seated lipid plugs using bio-mimetic enzymes that do not trigger transepidermal water loss. More crucially, the core of the service involves an aggressive "acidiculation" process. We deploy pH 4.5–5.5 botanical astringents that physically force the scalp's ecosystem back to a hostile state for pathogenic bacteria and fungi.
By restoring the structural integrity of the barrier and stripping away the excess liquefied sebum, we remove both the fuel and the environment required for an infection to take hold. Furthermore, by integrating vagus nerve stimulation to downregulate systemic stress, we reduce the cortisol spikes that additionally drive sebaceous overactivity, locking in a clear, highly resilient scalp capable of withstanding the Malaysian humidity.
Frequently Asked Questions
Q: Is "scalp acne" the same as the acne on my face? A: No. While facial acne (Acne Vulgaris) is heavily driven by the *Cutibacterium acnes* bacteria and severe hormonal fluctuations, scalp acne is almost entirely Scalp Folliculitis—an infection or inflammation mostly driven by *Staphylococcus aureus* bacteria or *Malassezia* fungus due to environmental heat, sweat occlusion, and compromised scalp barrier function.
Q: Why does my scalp get pimples when I wear a hijab all day? A: The microclimate under your hijab holds temperatures +2-4°C hotter than outside and traps humidity at 100%. This extreme wet heat degrades your scalp's protective acidic mantle while liquefying your sebum. The physical friction from your inner cap then rubs opportunistic bacteria directly into your unprotected hair follicles, causing widespread infection.
Q: Can I pop the pimples on my scalp to make them go away faster? A: Absolutely not. Popping a pustule on your scalp ruptures the walls of the infected hair follicle *underneath* your skin. This blasts millions of aggressive bacteria directly into the surrounding healthy dermis, rapidly spreading a small, single-pimple infection into a massive, deep, highly destructive boil that can permanently kill the hair root and leave a bald scar.
Q: How do I know if I need antibiotics for my scalp? A: If the bumps are extremely large, deeply painful (like hard marbles under the skin), spreading aggressively, causing the hair to permanently fall out in patches, or if you develop a fever or swollen lymph nodes, you have a severe, deep bacterial infection requiring immediate prescription antibiotics from a dermatologist. TTE handles superficial, recurrent environmental folliculitis.
***
References
- Luelmo-Aguilar, J., & Santandreu, M. S. (2004). *Folliculitis: recognition and management*. American Journal of Clinical Dermatology, 5(5), 301-310.
- Hald, M., Arendrup, M. C., Svejgaard, E. L., Lindskov, R., Foged, E. K., Saunte, D. M., & Danish Society of Dermatology. (2015). *Evidence-based Danish guidelines for the treatment of Malassezia-related skin diseases*. Acta Dermato-Venereologica, 95(1), 12-19.
- Chiller, K., Selkin, B. A., & Murakawa, G. J. (2001). *Skin microflora and bacterial infections of the skin*. Journal of Investigative Dermatology Symposium Proceedings, 6(3), 170-174.
- Yeo, S. P., & Hashim, H. (2019). *Prevalence and risk factors of scalp dermatoses among hijab-wearing women*. South East Asia Journal of Public Health, 9(1), 34-40.
