Postpartum hair loss in Malaysia is a profound source of psychological distress for new mothers. Experiencing intense, diffuse shedding—often losing clumps of hair in the shower or on the pillow—can be terrifying. However, clinically categorized as Postpartum Telogen Effluvium, it is not a sign of permanent destruction but rather a severe systemic disruption. Reassurance is vital: you are not going bald. However, ignoring the physiological shock can unnecessarily prolong the shedding phase for over a year.
Recovering effectively requires understanding the severe estrogen withdrawal mechanism, addressing the nutritional accelerants commonly found in Malaysian postnatal diets, and proactively managing the enormous cortisol load generated by newborn sleep deprivation.
What is the Oestrogen Withdrawal Mechanism?
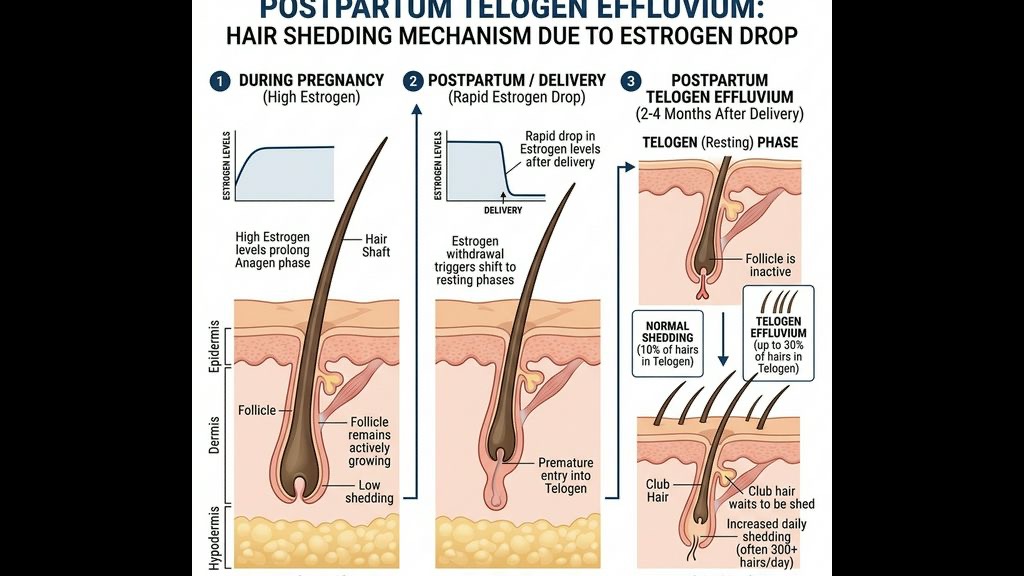
The foundation of postpartum shedding lies entirely within endocrinology. During pregnancy, the placenta secretes an enormous volume of circulating oestrogen and progesterone. High sustained levels of oestrogen essentially command the hair follicle to remain firmly locked in the anagen (growth) phase. Normally, human hair cycles through growth, resting, and shedding phases naturally. But pregnancy pauses the final shedding (telogen) phase entirely. This is why many women experience their thickest, most lustrous hair during the second and third trimesters.
Immediately following childbirth and the delivery of the placenta, systemic oestrogen levels plummet drastically within 48 to 72 hours. This enormous hormonal crash acts as a systemic "stop" signal to the hair follicles. It triggers a profound, synchronized shift.
Instead of the usual uncoordinated shedding where only 10% of hairs are resting at any given time, the oestrogen withdrawal forces up to 30–50% of the entire scalp's hair immediately into the telogen phase. Because the telogen phase takes approximately 100 to 120 days before the hair shaft actually detaches from the bulb and falls out, the massive shedding event typically peaks between Month 3 and Month 5 postpartum.
This delay—the fact that the hair loss begins months after the birth—often confuses new mothers who assume the trauma of the delivery directly caused the immediate shedding. It is pure hormonal synchronization. While it is physiologically "normal," the sheer volume of shedding frequently requires clinical management to ensure optimal recovery.
How Does Iron Deficiency Accelerate Postpartum Hair Loss?
The oestrogen crash guarantees the shedding will occur, but profound iron deficiency is the primary factor that prevents the hair from growing back rapidly. The biological demands of fetal development, combined with the often massive blood loss (hemorrhage) during parturition, leave most new mothers severely depleted of their iron reserves.
Iron is the most critical nutritional cofactor required by ribonucleotide reductase, the enzyme directly responsible for the massive DNA synthesis required by rapidly dividing hair matrix cells to create new hair shafts.
In clinical dermatology, a woman’s iron storage is measured via serum ferritin. To merely maintain a normal hair cycle without shedding, a minimum ferritin threshold of 30 µg/L is required. For active, robust hair regrowth—which a postpartum scalp desperately needs—ferritin levels frequently need to be pushed upwards of 70 µg/L.
Unfortunately, standard Malaysian postnatal practices occasionally worsen this deficit. While traditional confinement (pantang) soups are lauded, they often lack the bioavailable heme iron volume required to drag a severely depleted mother’s ferritin back to 70 µg/L rapidly. The body is in strict survival mode. If iron is scarce, the biological triage system immediately shuts off completely "unnecessary" functions like hair regeneration to divert what meager iron remains to vital organ function and breast milk production. The result is prolonged, unrecoverable thinning.
Why Do Sleep Deprivation and Cortisol Prolong the Shedding?
Beyond the biological nutrient drain, a newborn creates a devastating neurological load characterized by chronic, severe sleep deprivation.
The hair follicle is acutely sensitive to human Growth Hormone (GH), a peptide hormone that strongly stimulates the anagen (growth) phase. However, adult GH is secreted almost entirely in pulsatile bursts during the first few cycles of deep, slow-wave sleep. When a Malaysian mother’s sleep is shattered every two to three hours for feeding or settling, she never enters sufficient deep slow-wave sleep. Consequently, her nightly Growth Hormone production crashes.
Simultaneously, the sheer exhaustion forces the Hypothalamic-Pituitary-Adrenal (HPA) axis into overdrive, causing cortisol to spike to sustain arousal during the day. Elevated cortisol binds directly to hair follicle receptors, suppressing the synthesis of the critical proteoglycans that anchor new hair into the scalp, and forcing whatever new hair tries to grow prematurely back into the telogen phase.
This dual insult—zero Growth Hormone and maximum cortisol—means the body fundamentally lacks both the chemical signal to grow hair and the cellular environment to sustain it. Prolonged, unmanaged cortisol load is what turns a standard 3-month postpartum shedding episode into chronic telogen effluvium that lasts up to 18 months.
How Does Breastfeeding Delay Hormonal Recovery?
Breastfeeding, while incredibly beneficial for the infant, demands specialized clinical support for the mother’s scalp. Exclusively breastfeeding mothers maintain extremely high circulating levels of prolactin—the necessary hormone for lactation.
Prolactin, however, strongly suppresses the ovaries' ability to resume normal cyclical oestrogen production. This prolonged suppression means the protective, hair-stimulating benefits of oestrogen are absent for an extended period. The scalp remains in a somewhat "hormonally dormant" state while the mother provides nutrition to the infant.
To offset this suppressed oestrogen, the scalp requires significantly more external support. Increased blood flow to the dermal papilla, removal of any follicular obstruction (like oxidized sebum buildup from irregular washing), and targeted delivery of topical nutrients become paramount precisely when the new mother has the least time to manage her personal care.
What is TTE’s Postpartum Scalp Restoration Protocol?
At TTE Elephant Head Spa, our dedicated [Postpartum Hair Loss](/concerns/postpartum-hair-loss) protocols acknowledge that you cannot simply scrub the hair back into existence with a "thickening" shampoo. Attempting to forcefully scrub a postpartum scalp often just rips out highly fragile hair shafts (traction).
Our intervention focuses on creating the ideal clinical runway for new anagen growth, while intensely managing the nervous system load. The protocol involves:
### 1. Zero-Traction Follicular Decalcification We utilize incredibly gentle, non-abrasive bio-active enzymes to perfectly clear the follicle ostia of built-up sebum and dead skin cells. This ensures that as the new, fragile vellus hairs begin to sprout from the dermal papilla, they do not encounter a microscopic wall of hardened, oxidized wax which forces them to buckle or fall out prematurely.
### 2. Vagus Nerve Activation for Cortisol Down-regulation The psychological core of our approach bridges the gap caused by the mother's sleep debt. Through specific, targeted occipital and kinetic compressions (nVNS), we mechanically suppress the sympathetic nervous system and activate the parasympathetic "rest and digest" pathway. This physically forces a temporary, massive drop in the mother's systemic cortisol load, providing the exhausted follicle a systemic break from stress signaling.
### 3. Intensive Dermal Microcirculation Enhancement Because her body is triaging nutrients away from her scalp, we must mechanically force the blood back to the surface. Clinical scalp manipulation and thermal differentiation treatments drastically increase the localized blood volume delivered to the dermal papilla. This ensures that whatever trace minerals and iron the mother is consuming are being actively driven to the hair roots where they are desperately needed for regrowth.
Experiencing postpartum hair loss is frightening, but it is highly responsive to proper, clinically targeted supportive care. Our goal is to shorten the shedding window and accelerate the return to density.
Frequently Asked Questions
Q: When does postpartum hair loss usually stop? A: Typically, the shedding begins around 3 to 4 months after childbirth and reaches its peak at 5 to 6 months. For most healthy women, it naturally resolves by their baby's first birthday. If it continues heavily past 12 months, you must check your iron (ferritin) and thyroid levels.
Q: Can I stop the hair from falling out once it starts? A: No, you cannot stop the initial shedding. Those hairs were hormonally programmed to fall the moment you gave birth. The goal of scalp treatments is *not* to glue dead hair back onto the scalp; it is to create the absolute optimal, low-inflammation environment to rapidly accelerate the *new* hair growing behind it.
Q: Why do I have so much dandruff after giving birth? A: The drastic shift in hormones changes the lipid composition of your sebum. Combined with less frequent hair washing (due to exhaustion) and elevated stress cortisol, your scalp pH shifts, allowing opportunistic *Malassezia* fungi to aggressively overpopulate and trigger dandruff and seborrhoeic dermatitis.
Q: Will a head spa damage my hair while it's falling out? A: No. A standard salon scrub might, but TTE's clinical postpartum protocol uses Zero-Traction cleansing. We use bio-enzymes to dissolve the sebum rather than aggressively scrubbing the fragile roots. Furthermore, the vagus nerve relaxation physically stops the stress loop driving longer-term hair loss.
***
References
- Piérard-Franchimont, C., & Piérard, G. E. (2013). *Alterations in Hair Follicle Dynamics in Women*. BioMed Research International, 2013, 1-6.
- Eastham, J. H. (2001). *Postpartum alopecia*. Annals of Pharmacotherapy, 35(2), 255-258.
- Trost, L. B., Bergfeld, W. F., & Calogeras, E. (2006). *The diagnosis and treatment of iron deficiency and its potential relationship to hair loss*. Journal of the American Academy of Dermatology, 54(5), 824-844.
- Sinclair, R. (2015). *Healthy Hair: What Is it?*. Journal of Investigative Dermatology Symposium Proceedings, 14(1), 2-5.
