Hair fall in Malaysia is predominantly driven by a combination of genetic susceptibility, elevated cortisol from high-stress commuting, and an aggressive tropical climate that disrupts the scalp microbiome. Treating diffuse shedding requires identifying the exact root cause—whether hormonal, nutritional, or stress-induced—rather than relying on generic topical serums.
Why Is Hair Fall Increasing Among Malaysian Urban Professionals?
The rapid urbanization of Malaysia over the last two decades has introduced unprecedented environmental and psychological stressors that directly impact scalp health. Data from the Malaysian Dermatological Society indicates that 1 in 3 Malaysian adults aged 25–44 reports significant hair fall, a statistic heavily weighted towards those working and residing in densely populated commercial zones.
In Kuala Lumpur specifically, the daily environmental load on a hair follicle is immense. The transition from 33°C outdoor heat into 19°C air-conditioned offices—repeated 2–4 times daily—creates a severe humidity swing. This repeated "barrier shock" disrupts the scalp's acid mantle significantly faster than what is observed in temperate climates. A compromised acid mantle accelerates moisture loss, forcing the sebaceous glands to overproduce sebum. This oxidised sebum traps heat and blocks follicles, prematurely forcing hair strands from the anagen (growth) phase into the telogen (resting) phase.
Furthermore, the psychological toll of urban commuting cannot be ignored. For professionals managing the daily JB–KL commute or navigating severe Causeway congestion, the chronic cortisol dysregulation is profound. Documented high-anticipatory-anxiety cortisol loads have been shown to directly suppress follicle stem cell activity. When cortisol remains elevated due to a 2.3-hour daily average commute, the body reallocates resources away from "non-essential" functions like hair growth, triggering mass shedding known as telogen effluvium.
To understand how to reverse this, we must first categorise hair fall into its five primary biological pathways.
What is Telogen Effluvium and How Does Stress Trigger Hair Loss?
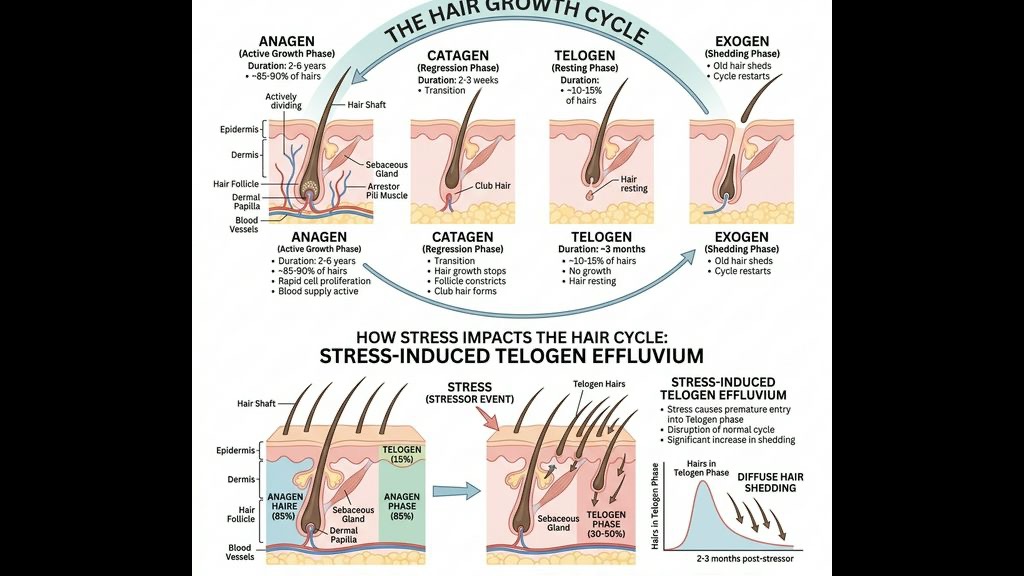
Telogen Effluvium (TE) is the most common cause of sudden, diffuse hair shedding. In a healthy scalp, about 85% to 90% of hair is in the anagen phase, while 10% to 15% is in the telogen phase. However, when the body experiences severe stress—such as prolonged cortisol elevation from the Malaysian hustle, a severe viral infection, or significant weight loss—up to 30% or more of hairs can be abruptly pushed into the telogen phase synchronously.
The mechanism involves the Hypothalamic-Pituitary-Adrenal (HPA) axis. When stress triggers the HPA axis, systemic cortisol spikes. Cortisol acts on the hair follicle by reducing the synthesis of crucial proteoglycans that anchor the hair shaft, and by upregulating substance P, a neuropeptide that induces neurogenic inflammation. Clinical studies (e.g., *Thom, 2016, Journal of Clinical and Investigative Dermatology*) have demonstrated how sustained cortisol directly limits the anagen phase duration.
Patients suffering from TE typically notice aggressive shedding—often 300+ hairs a day—about three to four months after the triggering event. It is essential to manage this systemic stress response. Interventions like vagus nerve stimulation have proven effective in lowering the cortisol load. If you are experiencing commuter anxiety or sleep deprivation, booking a [Sleep Healing Headspa](/sleep-healing) session is a critical step in resetting your autonomic nervous system and interrupting the cortisol-shedding cycle.
How Does DHT Cause Androgenetic Alopecia in Men and Women?
Androgenetic Alopecia (AGA) is the classic pattern hair loss, responsible for the vast majority of progressive thinning in both men and women. The primary culprit in AGA is Dihydrotestosterone (DHT), a potent androgen derived from testosterone via the enzyme 5-alpha reductase.
In genetically susceptible individuals, hair follicles in the frontal, vertex, and crown regions possess a higher density of androgen receptors. When DHT binds to these receptors, it triggers a cascade of intracellular events that progressively shorten the anagen phase of the hair cycle and decrease the size of the follicle itself—a process known as follicular miniaturisation. Over successive cycles, the terminal (thick) hairs are replaced by vellus (fine, unpigmented) hairs, and eventually, the follicle may cease producing hair entirely.
In women, female pattern hair loss presents slightly differently, often sparing the frontal hairline and presenting as diffuse thinning along the midline part. While anti-androgen therapies are common medical interventions, maintaining an optimal scalp environment is crucial for slowing AGA progression. Excess sebum accumulation, which is rampant in Malaysia's 80–90% RH year-round humidity, concentrates DHT directly on the scalp surface, accelerating miniaturisation. Therefore, deep clinical cleansing of the follicle ostia is critical to prevent sebum stagnation from worsening the local hormonal load. Finding a reliable [head spa in Kuala Lumpur](/headspa-kl) that focuses on deep follicular cleansing can significantly mitigate this environmental accelerant.
Why Do New Mothers Experience Severe Postpartum Hair Loss?
Postpartum hair loss, medically known as postpartum telogen effluvium, is a highly distressing but physiologically predictable event for many Malaysian mothers. During pregnancy, elevated levels of oestrogen essentially freeze hair follicles in the anagen (growth) phase. This prevents normal daily shedding, resulting in the characteristic thick, lustrous hair of the second and third trimesters.
However, immediately following childbirth, oestrogen levels plummet dramatically. This hormonal withdrawal triggers a mass-synchronisation event where all the hairs that were artificially kept in the anagen phase transition into the telogen phase simultaneously. Approximately three to five months postpartum, the new mother may lose up to 30% of her hair volume in a matter of weeks.
This shedding is often compounded by the extreme physical fatigue of caring for a newborn. Sleep deprivation prevents the nocturnal secretion of Growth Hormone (GH)—which peaks during deep slow-wave sleep—further impairing follicle recovery. Furthermore, giving birth depletes the body's iron stores, a critical cofactor for hair synthesis. Reassurance is vital here: the hair follicle is not dead; it is merely heavily fatigued. A thorough [Postpartum Hair Loss](/concerns/postpartum-hair-loss) recovery protocol that addresses follicle stimulation, scalp nutrient delivery, and nervous system support can significantly shorten the shedding window.
Can Iron Deficiency and Poor Nutrition Accelerate Hair Fall?
Hair formation is one of the most metabolically demanding processes in the human body. The rapidly dividing matrix cells in the hair bulb require a constant supply of specific nutrients. When the body faces a nutritional deficit, it triages its resources, abandoning hair growth to preserve essential organ function.
Iron deficiency is the leading nutritional cause of hair loss, particularly in premenopausal women. Iron is required by the enzyme ribonucleotide reductase, which is essential for DNA synthesis during the rapid cell division of the hair follicle. Even without clinical anemia, low iron storage (measured as serum ferritin) can trigger profound hair shedding. Dermatological consensus dictates that a minimum ferritin threshold of 30 µg/L is required to maintain the normal hair cycle, while levels closer to 70 µg/L may be needed to achieve complete regrowth indicating why borderline levels lead to chronic shedding (Trost et al., 2006, Journal of the American Academy of Dermatology).
Beyond iron, deficiencies in Vitamin D, Zinc, and essential amino acids also disrupt the hair cycle. Modern Malaysian urban diets, which rely heavily on ultra-processed foods, often lack the trace minerals required for optimal follicle function. When combined with the high oxidative stress of the urban environment, this nutritional deficit severely compromises the scalp's ability to regenerate strong terminal hairs.
How Does Scalp Inflammation and Traction Destroy Follicles?
The fifth major pathway of hair loss involves direct physical or immunological destruction of the follicle. One highly relevant form of this in Malaysia is Traction Alopecia, prevalent among women who wear hijabs intricately styled or tightly pinned over a long period. The constant tension on the hair shaft, especially along the frontal and temporal hairlines, causes mechanical micro-trauma to the follicle. This chronic physical stress induces localized perifollicular inflammation, which can eventually lead to irreversible scarring.
Additionally, the microclimate under a hijab—characterised by a +2–4°C temperature rise and humidity trapping—creates a perfect incubator for microbial overgrowth. If you want to learn more about mitigating occlusion-induced inflammation, reading our [Hijabi Scalp Care](/concerns/hijabi-scalp-care) overview is highly recommended.
Moreover, severe systemic or local scalp inflammation—such as seborrheic dermatitis or neurogenic scalp itch—recruits immune cells that release pro-inflammatory cytokines like IL-1α and TNF-α. These cytokines are potent inhibitors of hair growth and directly force follicles prematurely into the telogen phase. Treating hair loss under these conditions without first extinguishing the inflammation is akin to planting seeds in a burning field.
Why is Trichoscopy the Golden Standard for Hair Loss Diagnosis in Malaysia?
Because the five biological pathways of hair loss often overlap—for instance, a woman could be experiencing concurrent Androgenetic Alopecia, Telogen Effluvium from work stress, and mild Iron deficiency—a visual inspection alone is completely inadequate for a proper diagnosis.
- Hair shaft thickness variability: A hallmark of Androgenetic Alopecia (miniaturisation).
- Empty follicles with yellow dots: Indicative of severe sebaceous buildup or prolonged Alopecia Areata.
- Perifollicular erythema (redness around the base of the hair): Suggests active inflammation or early scarring alopecia.
- Predominance of single hair follicular units: Suggests progressive shedding instead of multi-hair groupings typical in a dense scalp.
Relying on "feeling" the scalp or simply observing shed hairs on a brush cannot provide this critical differentiation. Trichoscopy precisely dictates whether the intervention must focus on sebum regulation, fungal eradication, hormonal buffering, or stress modulation.
What Does TTE Elephant Head Spa’s Clinical Recovery Protocol Involve?
At TTE Elephant Head Spa, our approach to mitigating hair loss transcends cosmetic smoothing and tackles the root biological distress. The treatment for [Hair Fall & Thinning](/concerns/hair-fall) is not a generic application, but a staged clinical intervention based on trichoscopic findings.
1. Complete Barrier Decalcification and Scaling: Using micro-exfoliation techniques that respect the acid mantle, we remove the oxidized sebum plugs, DHT accumulation, and environmental particulate matter deeply lodged within the follicle ostia. 2. Pathogen and Inflammation Control: If the shedding is complicated by Malassezia overgrowth or neurogenic itch, we apply targeted antimicrobial and anti-inflammatory botanicals to reset the surface ecology. 3. Autonomic Nervous System Down-regulation: Recognising the severe role of cortisol in the Malaysian urban landscape, our protocol integrates physiologically driven mechanoreceptor stimulation. Applying precise kinetic pressure across the occipital ridge mechanically stimulates vagus nerve afferents, driving the body from sympathetic "fight or flight" into parasympathetic "rest and digest," actively lowering the systemic cortisol load. 4. Follicular Blood Flow Enhancement: Improved microcirculation ensures that whatever nutrients the body has triaged are delivered efficiently directly to the dermal papilla.
Recovering from hair fall is a timeline measured in months, not days. However, establishing a clinically pristine scalp environment and shutting down local inflammation is the absolute prerequisite for any future regrowth.
Frequently Asked Questions
Q: Why do I lose more hair when I am stressed from work in KL? A: Chronic work stress elevates systemic cortisol levels. Cortisol acts directly on the hair follicle to suppress the synthesis of proteoglycans, prematurely pushing growing hairs into the shedding (telogen) phase. The average commuter stress in the KL and JB zones can significantly worsen this response.
Q: Can a head spa actually help with postpartum hair loss? A: Yes, while the hormonal drop is an inevitable physiological process, a head spa aids recovery significantly. It clears the scalp of accumulating sebum, prevents secondary inflammation, and provides critical nervous system support to mitigate the sleep deprivation stress that prolongs shedding.
Q: Is it normal to see 100 hairs fall out when washing my hair in Malaysia? A: Losing 50-100 hairs daily is normal shedding. However, if this volume consistently increases or you notice simultaneous widening of your hair parting, it indicates advanced telogen effluvium or androgenetic thinning. A trichoscopic evaluation is required to identify the root cause.
Q: What is the best treatment for diffuse hair fall in Malaysia? A: The most effective long-term treatment involves managing the internal triggers (like stress or iron levels) combined with advanced clinical scalp cleansing. The TTE protocol thoroughly resets the scalp microbiome, clears follicular obstructions, and directly down-regulates the stress pathways via targeted neurological relaxation, providing the ideal foundation for hair recovery.
***
References
- Thom, E. (2016). *Stress and the Hair Growth Cycle: Cortisol-Induced Hair Growth Disruption*. Journal of Clinical and Investigative Dermatology, 4(1), 1-6.
- Trost, L. B., Bergfeld, W. F., & Calogeras, E. (2006). *The diagnosis and treatment of iron deficiency and its potential relationship to hair loss*. Journal of the American Academy of Dermatology, 54(5), 824-844.
- Misery, L., Sibaud, V., Ambonati, M., Macy, G., Boussetta, S., & Taieb, C. (2008). *Sensitive scalp: does this condition exist? An epidemiological study*. Contact Dermatitis, 58(4), 234-238.
- Kanti, V., Messenger, A., Dobos, G., Reygagne, P., Finner, A., Blumeyer, A., ... & Blume-Peytavi, U. (2018). *Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men*. Journal of the European Academy of Dermatology and Venereology, 32(1), 11-22.
