Male pattern baldness is not a vanity concern. It is a progressive biological process driven by a hormone your body produces in increasing quantities from your mid-twenties onward. Left unaddressed, it follows a predictable miniaturisation cascade that cannot be reversed once follicles reach terminal atrophy.
The science is well-established. The intervention options are effective — if deployed early enough. What most Malaysian men lack is not access to treatment but an accurate understanding of the timeline they are working against.
The DHT Conversion Pathway
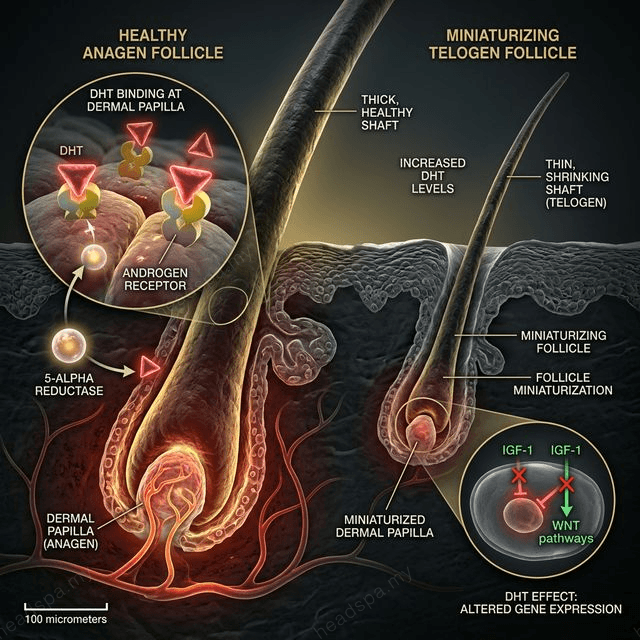
Testosterone circulates in the bloodstream in relatively hair-safe concentrations. The problem is its conversion. The enzyme 5α-reductase (5-AR), present in high concentrations in scalp dermal papilla cells, converts testosterone into dihydrotestosterone (DHT) — an androgen that is three to five times more potent than testosterone and has a much higher affinity for the androgen receptor (AR) at the follicle.
When DHT binds to the AR in genetically susceptible follicles, it initiates a signalling cascade that progressively shortens the anagen (growth) phase. A follicle that once cycled through a three-year anagen phase — producing a long, terminal hair — begins cycling through progressively shorter phases: two years, then one year, then months. With each shortened cycle, the hair shaft produced is finer and shorter. The follicle miniaturises.
Over a decade, a follicle that was producing a full-diameter terminal hair shaft is producing a vellus hair — fine, depigmented, cosmetically invisible. The follicle is still alive at this stage, but it has reached functional obsolescence. This is why intervention timing is the single most important variable in androgenetic alopecia management.
Malaysian Genetic Context
Southeast Asian male populations — including Malaysian Chinese, Malay, and Indian ethnic groups — exhibit distinct androgen sensitivity profiles relative to European populations. Studies on Asian hair follicle physiology document higher 5-AR type II activity in scalp tissue, meaning that for equivalent testosterone levels, DHT conversion at the follicle is proportionally greater.
This does not mean baldness is inevitable earlier. It means the sensitivity to DHT-mediated miniaturisation is higher, and the intervention window — the period during which early-stage follicles can be preserved and late-stage atrophy can be delayed — requires earlier clinical attention than European-derived guidelines would suggest.
Family history on the maternal side (X-chromosome AR gene inheritance) remains the strongest single predictor of androgenetic alopecia severity and onset age.
The Norwood Classification
The Hamilton-Norwood scale provides the clinical framework for staging androgenetic alopecia progression and selecting interventions appropriate to each stage.
| Norwood Stage | Pattern Description | Intervention Urgency | |---|---|---| | I | Minimal to no recession; mature hairline | Monitoring; lifestyle optimisation | | II | Slight temporal recession; triangular recession zones | Low urgency; topical minoxidil optional | | III | Deeper temporal recession; vertex thinning may begin | Moderate; initiate treatment | | III Vertex | Significant crown thinning with preserved frontal line | High; dual-target treatment indicated | | IV | Hairline recession + dense crown loss; bridge of hair separating | High; systemic options indicated | | V | Bridge narrows; frontal and crown regions merging | Urgent; maximise pharmacological intervention | | VI–VII | Extensive loss; only posterior/lateral band remains | Surgical candidacy assessment |
The critical clinical insight is that most Malaysian men first seek treatment at Norwood III–IV — a stage where significant follicle atrophy has already occurred. Intervention at Norwood I–II preserves substantially more follicular capital.
Why Starting Early Determines Outcome
The miniaturisation process is not reversible once a follicle has completed terminal atrophy. What pharmacological and supportive interventions do is slow the progression rate and extend the productive life of follicles that are mid-miniaturisation — not regenerate follicles that have completed the process.
This means a man who begins intervention at Norwood II retains meaningfully more density at Norwood IV than a man who begins at Norwood IV. The follicle reservoir is finite. Every year of unmanaged DHT exposure at sensitive follicles reduces the ceiling of what treatment can achieve.
Clinical Intervention Options
Minoxidil (topical or oral): A vasodilator that increases blood flow to the follicle and prolongs the anagen phase. Does not block DHT — it compensates by extending the productive phase of miniaturising follicles. Requires continuous use; discontinuation results in resumed miniaturisation within months. Most effective at Norwood II–III.
Finasteride (oral) / Dutasteride: 5-AR inhibitors that block DHT conversion at the enzyme level. Finasteride inhibits 5-AR type II; dutasteride inhibits both type I and II. Reduces serum DHT by 60–70% (finasteride) or up to 90% (dutasteride). Most effective pharmacological intervention available; requires dermatology prescription and monitoring. Side effect profile should be discussed with a physician before initiation.
Low-Level Laser Therapy (LLLT): Photobiomodulation that stimulates mitochondrial activity in follicle cells, extending anagen and improving cellular energy metabolism. Evidence base is moderate; most effective as an adjunct to pharmacological treatment. Available at our [KL](/headspa-kl) and [JB](/headspa-jb) locations as part of the trichoscopy-guided treatment protocol.
Trichoscopy monitoring: At TTE Elephant, scalp assessment via trichoscopy provides quantified data on follicle miniaturisation percentage, hair density per cm², and anagen-to-telogen ratio. This removes guesswork from the intervention timeline and creates an objective baseline for measuring treatment response over six-to-twelve month intervals.
Scalp circulation support: Androgenetic alopecia is associated with reduced microvascular density at the vertex and frontal scalp — the zones of highest DHT sensitivity. Regular scalp massage protocols demonstrably increase blood flow to the follicle papilla, supporting nutrient and oxygen delivery. This does not reverse DHT-mediated miniaturisation, but it optimises the microenvironment for any concurrent pharmacological intervention.
The [hair fall assessment at TTE Elephant](/concerns/hair-fall) is the appropriate starting point for any man concerned about temple recession or crown thinning. Staging precedes treatment selection. Treating without staging is guessing.
---
Q: Does wearing hats cause hair loss in Malaysian men? A: No. Hat-wearing does not cause androgenetic alopecia. DHT sensitivity is the driver — not scalp occlusion, compression, or sweat accumulation from headwear. If thinning correlates with hat use, the timing is coincidental with the natural progression of androgenetic alopecia, not causal.
Q: At what age should Malaysian men start monitoring for male pattern baldness? A: If there is a family history of androgenetic alopecia — particularly on the maternal side — monitoring should begin at age 20–22. A trichoscopy baseline at this age provides a reference density map. Even if no intervention is needed immediately, having a baseline allows objective measurement of miniaturisation rate when signs do appear, rather than relying on subjective recall.
Q: Is androgenetic alopecia reversible? A: Miniaturisation is not reversible once a follicle reaches terminal atrophy. However, follicles in the mid-miniaturisation process — the majority of affected follicles in Norwood II–IV — can be stabilised and their productive life extended significantly through DHT blockade and vascular support. The earlier intervention begins, the greater the proportion of follicles that can be preserved.
Q: Can head spa alone stop male pattern baldness? A: No. Androgenetic alopecia requires pharmacological DHT intervention to halt its core mechanism. Head spa — including scalp massage, LLLT, and trichoscopy monitoring — is a clinically valid adjunct that optimises the follicle microenvironment, reduces inflammatory co-factors, and tracks progression. It amplifies the effectiveness of medical treatment; it does not replace it.
