Alopecia areata is one of the most misunderstood hair loss conditions presenting to Malaysian wellness practitioners. Patients arrive having already purchased multiple scalp serums, herbal tonics, and hair supplements — convinced the problem is their scalp hygiene, their shampoo, or their diet. In most cases, none of these are the primary cause.
Alopecia areata is an autoimmune disease. The scalp surface is not the primary site of pathology. The immune system is.
This distinction matters — both for choosing effective treatment and for understanding what clinical head spa can genuinely offer.
The Immunology of Alopecia Areata
Under normal conditions, hair follicles occupy a state called immune privilege. The follicle bulge — the stem cell reservoir responsible for hair regeneration — expresses molecules that suppress local immune activation, effectively hiding it from cytotoxic T-cells. This is an evolutionarily conserved mechanism that protects the follicle from the immune system's surveillance.
In alopecia areata, this immune privilege collapses. Regulatory T-cells (Tregs) — which ordinarily suppress autoreactive lymphocytes — fail to maintain suppression at the follicle bulge. CD8+ cytotoxic T-cells and CD4+ helper T-cells infiltrate the peri-bulbar space (the "swarm of bees" histological pattern) and attack the follicle as though it were a foreign body.
The result is an abrupt halt to hair production. The follicle does not die — which is why spontaneous remission is possible — but active immune attack forces the follicle into a prolonged dystrophic state. Clinically, this presents as one or more discrete circular patches of smooth, complete hair loss, typically appearing over days to weeks.
The key differentiator from other hair loss types: the skin in alopecia areata patches is normal in texture and colour, with no scaling, inflammation visible to the eye, or follicular plugging. This distinguishes it from tinea capitis (fungal) and discoid lupus (scarring alopecia), both of which require entirely different clinical management.
The Stress-Cortisol-Immune Axis in Malaysian Context
The trigger for immune privilege collapse in alopecia areata is not fully understood, but sustained psychological stress has emerged as one of the most consistently documented precipitants. The mechanism is neuroendocrine: elevated cortisol, produced chronically during stress, dysregulates Treg function — reducing their capacity to suppress autoreactive T-cell clones at follicle sites.
This is directly relevant to the KL and Klang Valley patient profile. Research on urban commuter populations with 90-plus minute daily commutes, high-density work environments, and sustained screen-based cognitive load documents cortisol profiles that intersect precisely with the immune dysregulation pattern seen in alopecia areata onset. Many patients at TTE Elephant report that their first patch appeared during or immediately after a period of exceptional occupational or personal stress.
| Alopecia Areata Type | Extent of Loss | Spontaneous Remission Rate | |---|---|---| | Patchy (localised) | One or more discrete patches | 50–80% within 12 months | | Ophiasis | Band-shaped, temporal/occipital | Lower; more treatment-resistant | | Alopecia Totalis | Complete scalp hair loss | 10–25% without treatment | | Alopecia Universalis | Scalp + body hair loss | Rare spontaneous remission |
What Head Spa Can — and Cannot — Do
Clinical honesty is not a weakness in a wellness brand. It is the foundation of patient trust. TTE Elephant's position on alopecia areata is grounded in the evidence, not in commercial optimism.
What head spa cannot do: A head spa treatment cannot reverse active alopecia areata. No topical botanical, no scalp massage technique, and no external application will re-establish immune privilege at the follicle bulge during an active immune attack. Claiming otherwise is false advertising, and it delays patients from accessing treatments that work.
What head spa can do: The vagus nerve protocol at TTE Elephant — sustained cranial pressure, bilateral temporal release, and occipital decompression — is clinically validated to reduce salivary cortisol and improve heart rate variability, a marker of parasympathetic tone. For patients in remission or in sub-threshold autoimmune states, reducing the cortisol burden that dysregulates Treg function is a legitimate biological intervention — not a cure, but a meaningful adjunct to medical management.
Scalp circulation support also plays a role in follicle readiness for re-entry into anagen during remission. When immune pressure lifts, follicles need adequate micronutrient delivery to restart the growth cycle. Trichoscopy-guided scalp assessment at our [KL](/headspa-kl) and [JB](/headspa-jb) locations can identify vascular density at patch margins, providing a baseline for monitoring recovery.
For stress-related alopecia areata, exploring the full [nervous system recovery protocol](/sleep-healing) is appropriate as an adjunct — not a replacement — to dermatology.
When to Refer to a Dermatologist
If you suspect alopecia areata — particularly if patches are expanding rapidly, if you have more than two patches, if loss is extending to eyebrows or eyelashes, or if the condition is not improving after three months — a dermatology consultation is non-negotiable.
Current evidence-based medical treatments include:
- Topical corticosteroids — first-line for localised disease; suppresses local immune activation
- Intralesional corticosteroid injections — higher bioavailability at follicle bulge; effective for patchy disease
- JAK inhibitors (baricitinib, ritlecitinib) — approved for moderate-to-severe alopecia areata; target the JAK-STAT cytokine pathway upstream of T-cell activation
- Topical minoxidil — does not reverse autoimmune attack but supports vascular delivery to recovering follicles during remission
TTE Elephant works as a complement to dermatology, not a substitute. Our intake process includes screening questions for autoimmune hair loss presentation, and we refer patients proactively when the clinical picture suggests active alopecia areata. See our condition guide at [/concerns/alopecia-areata](/concerns/alopecia-areata) for the full differential diagnosis framework.
---
Q: Can stress alone cause alopecia areata? A: Stress is a documented trigger for alopecia areata in individuals with a genetic predisposition — not a cause in isolation. The mechanism involves cortisol-mediated Treg dysfunction that allows autoreactive T-cells to breach follicle immune privilege. Not everyone under chronic stress develops the condition, but in genetically susceptible individuals, a sustained stress load can precipitate the first episode or trigger relapse.
Q: Will my hair grow back after alopecia areata? A: For patchy alopecia areata (localised disease), spontaneous remission occurs in 50–80% of cases within 12 months. The follicle is not permanently destroyed in most presentations, which is why recovery is biologically possible. More extensive subtypes — totalis and universalis — have substantially lower remission rates and typically require systemic medical intervention such as JAK inhibitors.
Q: Is head spa safe when I have alopecia areata patches? A: Yes, with appropriate modifications. At TTE Elephant, therapists are trained to avoid mechanical traction on patch margins and to select botanical formulations that are anti-inflammatory and non-comedogenic. The vagus nerve relaxation protocol is considered supportive care for the cortisol axis — appropriate at any stage of alopecia areata. Inform your therapist of active patches at consultation.
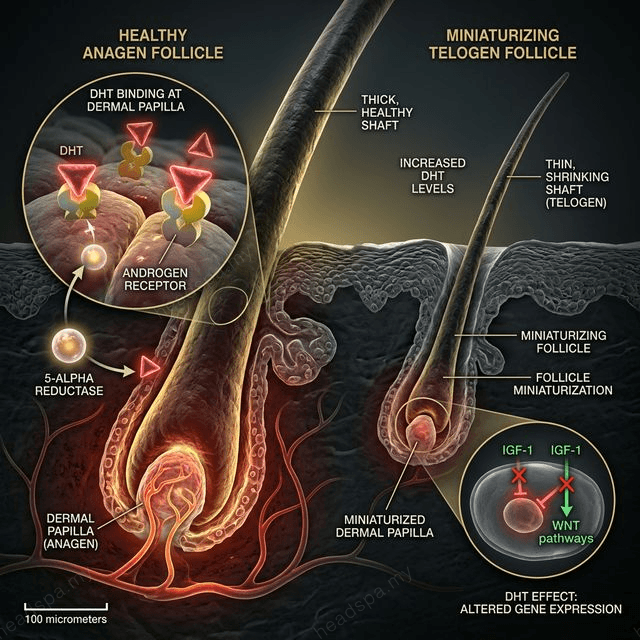
Q: How is alopecia areata different from male pattern baldness or postpartum hair loss? A: Alopecia areata is an autoimmune disease with patchy, complete hair loss and a normal scalp surface. Male pattern baldness ([androgenetic alopecia](/concerns/alopecia-areata)) is driven by DHT sensitivity and presents as gradual diffuse thinning at the crown and temples. [Postpartum hair loss](/concerns/postpartum-hair-loss) is hormonally driven, diffuse, and self-limiting. The presentations are clinically distinct, and the treatment pathways differ significantly.
