Alopecia areata is perhaps the most psychologically devastating form of hair loss because of its abrupt, unpredictable onset. Often discovered completely by accident—by a barber or while running fingers through the hair—the sudden appearance of a perfectly smooth, completely bald circular patch on the scalp invokes immediate panic.
In Malaysia, managing Alopecia Areata requires a starkly honest clinical approach. It is an autoimmune condition. It cannot be "cured" by rubbing ginseng tonic or commercial ginger extract onto the bald spot. True clinical support involves understanding the immune collapse, managing the intense psychological stress that often triggers it, and knowing exactly when to utilize a clinical head spa versus when to seek aggressive steroidal intervention from a dermatologist.
What is Alopecia Areata and Why Does it Happen?
To understand Alopecia Areata, you must first understand a fascinating evolutionary concept called "Immune Privilege."
In a healthy human body, the lower portion of the actively growing hair follicle (the anagen bulb) operates outside the jurisdiction of the body's immune system. Essentially, the body builds a chemical and physical wall around the follicle, preventing immune cells like T-lymphocytes from "seeing" the various proteins (autoantigens) produced during rapid hair synthesis.
Alopecia Areata is the catastrophic collapse of this immune privilege.
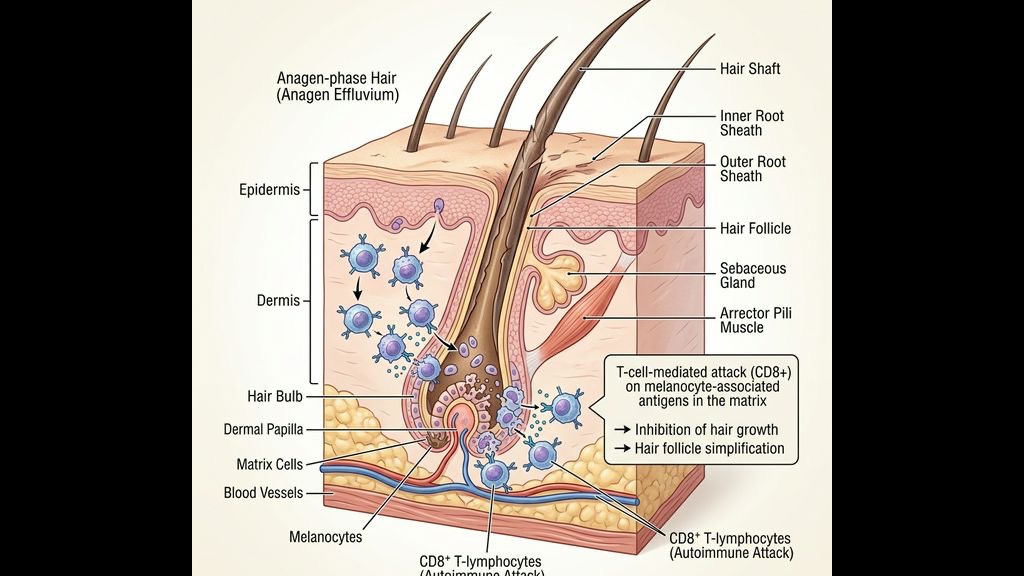
For reasons involving a mix of genetic predisposition and environmental triggers, the protective wall falls. Specifically, the follicle begins to express a distress signaling protein called NKG2D ligand. The body's own cytotoxic CD8+ T-cells detect this signal, misidentify the growing hair follicle as a dangerous foreign pathogen, and launch a massive, coordinated attack.
This inflammatory swarm forces the follicle to instantly abort the anagen (growth) phase. The hair shaft snaps or disconnects from the dermal papilla, resulting in the sudden, rapid shedding characteristic of the condition. Crucially, the immune system does *not* destroy the follicle's stem cells in the bulge region. The factory is simply shut down, not demolished. This means that if the inflammation can be suppressed, the hair can entirely regrow.
How Does Severe Stress Act as a Clinical Trigger?
While the underlying mechanism is immunological, the precipitating event—the spark that drops the protective wall—is very frequently severe psychological or physiological stress.
In the high-pressure environments of Kuala Lumpur and Johor Bahru, chronic stress is endemic. The biological bridge between "feeling stressed" and "immune collapse" is the Hypothalamic-Pituitary-Adrenal (HPA) axis. When you experience intense anxiety—whether from a major devastating life event or the chronic, grinding cortisol load of a 2.3-hour daily JB-KL commute—the hypothalamus releases Corticotropin-Releasing Hormone (CRH).
Research has explicitly shown that hair follicles possess their own localized, fully functional HPA-axis equivalent. Under extreme stress, CRH is synthesized directly within the skin. This triggers a massive influx of Substance P and mast cell degranulation around the follicle. This neurogenic inflammatory storm alters the localized immune microenvironment, effectively "unmasking" the follicle to the circulating T-cells waiting to attack.
The relationship is unfortunately bidirectional. The stress of the commute triggers the bald patch; discovering the bald patch triggers immense panic and further cortisol spikes; that new cortisol fuels the expansion of the patch or causes new ones to form. Breaking this central stress loop is as critical as treating the skin itself.
What Are the Spontaneous Remission Rates?
- Mild Alopecia Areata: One or two small patches (less than 25% of scalp coverage).
- Alopecia Totalis: Complete loss of all hair on the scalp.
- Alopecia Universalis: Complete loss of all hair on the entire body.
For the most common presentation—mild, patchy alopecia areata—the clinical statistics offer significant hope. Roughly 50% of patients with mild, limited patching will experience spontaneous remission (the hair grows back entirely on its own) within 12 months, without any medical intervention, provided the underlying stress trigger has resolved.
However, predicting *who* will spontaneously recover and who will progress to more severe forms is currently impossible. This uncertainty dictates the treatment methodology: we cannot guarantee it won't spread, so we must proactively suppress the localized inflammation and strictly manage the systemic cortisol load.
The Clinical Divide: When to See a Dermatologist vs. a Head Spa
At TTE Elephant Head Spa, transparency regarding our scope of practice is absolute. A head spa is not a medical clinic; we do not dispense intralesional corticosteroid injections or prescribe JAK inhibitors—these are potent, aggressive immunosuppressants requiring a licensed dermatologist.
- You are losing your eyebrows, eyelashes, or body hair.
- The patches are rapidly multiplying and joining together (coalescing) over a matter of weeks.
- The condition affects the edges of your hairline (Ophiasis pattern), which is notoriously difficult to treat and requires immediate strong medical suppression.
- You have small, stable patches and are opting to wait for spontaneous remission but need proactive environmental management.
- You are concurrently seeing a dermatologist for steroid treatments, but the injections are causing severe localized scalp atrophy (thinning of the skin) and dryness, requiring biomimetic lipid repair.
- The primary trigger of your outbreak was undeniably severe psychological stress or trauma, necessitating profound nervous system regulation.
How TTE Supports Alopecia Areata Recovery
Treating [Alopecia Areata](/concerns/alopecia-areata) requires a highly specialized, non-aggressive approach. The scalp is actively under an autoimmune siege; scrubbing it with commercial exfoliants or subjecting it to harsh thermal styling will massively exacerbate the T-cell infiltrate.
Our clinical protocol functions as a targeted support system to maximize the probability of remission:
### 1. High-Magnification Trichoscopy Monitoring We do not treat blindly. We utilize 200x magnification trichoscopy to monitor the affected patches. We specifically look for "exclamation mark hairs" (short hairs tapering at the base) which indicate the immune attack is still actively expanding, versus "yellow dots" (empty follicular ostia filled with sebum), or the appearance of fresh, unpigmented upright vellus hairs indicating remission has begun. This allows us to track real-time biological progress.
### 2. Deep Anti-Inflammatory Environmental Control The skin immediately surrounding the immune attack must be kept clinically pristine. We utilize ultra-gentle, pH 4.5–5.5 lipid cleansers to remove accumulated sebum without triggering any physical friction or barrier shock. Keeping the surrounding microbiome perfectly balanced ensures that secondary bacterial or Malassezia infections do not further aggravate the localized immune system.
### 3. Vagus Nerve Stimulated Cortisol Management This is our primary intervention. Because cortisol and CRH are the biological triggers sustaining the immune collapse, we must force the body's autonomic nervous system to downregulate. By applying sustained mechanical pressure to the occipital mechanoreceptors and activating the vagus pathways, our [Sleep Healing](/sleep-healing) integration physically forces a drop in systemic cortisol. We shut off the "alarm" signal so the body can repair the immune privilege wall.
It is a long journey, but understanding the biology changes the approach from blind panic to systematic recovery.
Frequently Asked Questions
Q: Did my stress cause this sudden bald patch? A: Stress is the most common precipitating trigger. While the underlying mechanism is an autoimmune attack (your immune cells attacking your hair), severe psychological stress heavily spikes cortisol and Corticotropin-Releasing Hormone (CRH), which effectively drops the protective barrier around your hair follicle, inviting the attack.
Q: Will the hair eventually grow back? A: Yes, for the majority of people with mild (one or two small patches) alopecia areata, there is a 50% chance the hair will spontaneously grow back within 12 months, even without strong medical treatment, because the follicle's stem cells are not permanently destroyed.
Q: Should I rub ginger or garlic on the bald patch to stimulate growth? A: Absolutely not. Ginger and garlic are strong contact irritants. Rubbing them raw on a scalp that is already suffering a severe inflammatory immune attack will cause Allergic Contact Dermatitis or a severe chemical burn, resulting in actual permanent scarring that guarantees the hair will never return.
Q: Can I do head spa treatments if I'm getting steroid injections at the clinic? A: Yes, they are highly complementary. While the dermatologist's steroids suppress the immune attack, our treatments focus on managing your systemic stress (the root trigger) and repairing the extreme scalp dryness and skin thinning that frequent steroid use often causes, creating the healthiest possible environment for the new hair to eventually surface.
***
References
- Gilhar, A., Etzioni, A., & Paus, R. (2012). *Alopecia areata*. New England Journal of Medicine, 366(16), 1515-1525.
- Peters, E. M., Liotiri, S., Bodó, E., Hagen, E., Lang, T., Fessing, M. Y., ... & Paus, R. (2007). *Probing the effects of stress mediators on the human hair follicle*. Brain, Behavior, and Immunity, 21(5), 716-727.
- Paus, R., Slominski, A., & Czarnetzki, B. M. (1994). *Is alopecia areata an autoimmune-response against follicles expressing growth-related autoantigens?*. Parasitology Today, 10(7), 239-242.
- Ito, T., Ito, N., Saatoff, M., Hashizume, H., Fukamizu, H., Nickoloff, B. J., ... & Paus, R. (2004). *Maintenance of hair follicle immune privilege is linked to prevention of NK cell attack*. Journal of Investigative Dermatology, 123(6), 1083-1090.
