Migraines and chronic tension headaches are often dismissed in corporate Malaysia as "just part of the job." However, this dismissal obscures a massive public health crisis. Approximately 15% of the Malaysian population—over 4.5 million adults—suffer from recurrent migraines. In high-density commercial hubs like Kuala Lumpur, the relentless combination of profound screen load, chronic posture distortion, and sheer commuter stress mechanically primes the neurological pathways for catastrophic pain.
Treating a severe migraine entirely with over-the-counter painkillers (NSAIDs) ignores the central neurological mechanism. The pain is not originating in the brain tissue itself (which has no pain receptors); it originates in the trigeminovascular system. Understanding how a clinically focused [head spa for migraine relief](/migraine-headache-relief-kl) interacts with this specific nervous system pathway reveals why mechanical scalp therapy is increasingly sought after as a powerful, non-pharmacological intervention.
What is the Trigeminovascular System and How Does KL Stress Prime It?
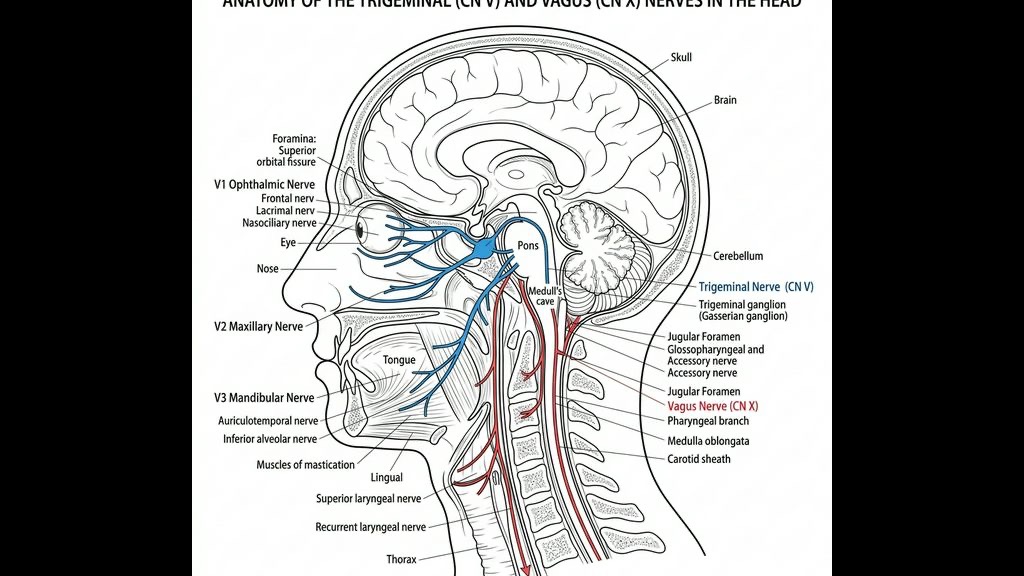
At the core of virtually every primary headache and migraine is the trigeminal nerve (Cranial Nerve V). This is the largest and most complex of the twelve cranial nerves, responsible for transmitting sensory information (touch, pain, temperature) from the face, scalp, and the meninges (the protective layers enveloping the brain) directly to the brainstem.
The trigeminovascular system refers specifically to the intricate network formed where the trigeminal nerve fibers wrap around the major cranial blood vessels. When an individual is exposed to a triggering event, these nerve endings become over-excited (depolarized) and dump massive quantities of potent vasoactive neuropeptides directly into the blood vessel walls.
For a professional in Kuala Lumpur, the "triggering events" are constant. 1. Screen Load and Photophobia: Staring at glaring monitors under fluorescent office lighting for 10 hours a day severely over-stimulates the ophthalmic branch (V1) of the trigeminal nerve. 2. Postural Distortion: Hunching over a laptop or gripping the steering wheel in intense Causeway or KL traffic causes sustained, tetanic contractions of the trapezius, splenius capitis, and suboccipital muscles at the base of the skull. This physical tension forcefully compresses the greater occipital nerve (which intertwines with the trigeminal system), essentially "priming" the entire trigeminocervical complex to misfire.
Why is CGRP the Bridge Between Migraines and an Itchy Scalp?
Of all the neuropeptides released during a migraine attack, none is more destructive—or more clinically targeted—than Calcitonin Gene-Related Peptide (CGRP).
When the trigeminal nerve fires, it releases a flood of CGRP. CGRP is an incredibly potent vasodilator; it forces the cranial blood vessels to rapidly, violently expand. This massive, sudden stretching of the vessel walls triggers the agonizing, pulsating, throbbing pain characteristic of a migraine. The role of CGRP is so undeniable that the newest, most expensive class of FDA-approved preventative migraine medications (like Aimovig or Emgality) are specifically designed as monoclonal antibodies that target and neutralize either CGRP itself or its receptor.
Fascinatingly, CGRP is the exact same neuropeptide centrally involved in neurogenic scalp inflammation. As detailed in our [Inflamed & Sensitive Scalp](/concerns/inflamed-sensitive-scalp) overview, when CGRP and Substance P are dumped into the scalp tissue by stressed nerve endings, they cause mast cells to degranulate, creating immense itching and burning *without* dandruff.
This is why nearly 40% of migraine sufferers report intense scalp sensitivity (allodynia) during an attack. Brushing the hair or wearing a tight hijab suddenly becomes excruciatingly painful. The same chemical (CGRP) is causing both the vasodilation inside the skull (the headache) and the inflammation on the skin outside the skull (the sensitive scalp).
How Does Vagus Nerve Stimulation (nVNS) Stop the Pain?
If the trigeminal nerve is the accelerator for a migraine, the Vagus nerve (Cranial Nerve X) is the emergency brake.
The Vagus nerve is the primary conduit for the parasympathetic nervous system (the "rest and digest" pathway). Modern neurology has discovered that artificially stimulating the Vagus nerve can forcefully suppress the excessive firing of the trigeminal nerve. The clinical validation for this is irrefutable: the FDA has approved non-invasive vagus nerve stimulators (like the gammaCore device) precisely for the acute treatment of episodic migraines and cluster headaches.
When the Vagus nerve is stimulated, it sends inhibitory signals into the trigeminal nucleus caudalis (the central relay station in the brainstem where headache pain is processed). This inhibitory signal physically blocks the trigeminal nerve from releasing further CGRP, stopping the vasodilation and halting the pain pathway. Furthermore, vagal tone is bidirectionally linked with sleep. Poor sleep triggers migraines, and migraines prevent deep sleep. Re-establishing high vagal tone is critical to resetting this destructive [Poor Sleep & Stress](/concerns/poor-sleep-stress) cycle.
What is TTE’s Occipital Ridge Protocol for Migraine Relief?
While electronic nVNS devices use mild electrical currents, the Vagus nerve can also be accessed mechanically. The auricular branch of the Vagus nerve (Arnold's nerve) innervates parts of the ear, while dense networks of mechanoreceptors at the base of the skull (the occipital ridge) communicate deeply with vagal afferent pathways.
At TTE Elephant Head Spa, our [Migraine & Tension Headache](/concerns/migraine-tension-headache) protocol is definitively not a superficial "rub." It is a targeted, mechanoreceptor-driven intervention.
### 1. Occipital Neural Release Using precise, sustained kinetic pressure, our specialists target the suboccipital triangle and the epicranial aponeurosis. This deep tissue mobilization forcefully breaks down the fascial adhesions caused by KL commuter posture. By physically releasing the structural compression on the greater occipital nerve, we remove the mechanical "primer" that continuously aggravates the trigeminocervical complex.
### 2. Mechanically Mediated nVNS Through highly specific rhythms of compression around the auricular pathways and the posterior cervical spine, we actively stimulate the parasympathetic rest response. This physically mimics the mechanism of an nVNS device, leveraging the body’s own anatomy to downregulate sympathetic drive, lower systemic cortisol, and suppress further CGRP dumping.
### 3. Thermal Contrast Decongestion We utilize precise thermodynamic shifts. Applying targeted thermal cooling to the scalp physically constricts the excessively dilated superficial blood vessels, providing immediate, profound relief from the throbbing sensation, while simultaneous warming of the cervical spine encourages total muscular relaxation.
It is crucial to state that a head spa is not an emergency room. If you are experiencing sudden, "thunderclap" headaches, or headaches accompanied by a loss of vision, limb numbness, or slurred speech, you must immediately seek emergency neurological medical care.
However, for the millions of Malaysians battling chronic tension headaches, screen-induced migraines, and the agonizing scalp sensitivity that accompanies them, integrating clinical, vagally-mediated scalp therapy offers an incredibly powerful, medication-free pathway back to clarity and pain-free focus.
Frequently Asked Questions
Q: Can a head spa really cure my migraines? A: A head spa is not a medical "cure" for the genetic predisposition to migraines. However, for many individuals, chronic migraines are continuously triggered by severe neck/scalp muscle tension and extremely high stress (which elevates cortisol and CGRP). A clinical head spa physically releases that muscular compression and actively stimulates the vagus nerve to lower the stress response, dramatically reducing the frequency and severity of the attacks.
Q: Why does my scalp hurt so much when I have a migraine? A: This is called cutaneous allodynia. During a migraine, the trigeminal nerve is hyperactive and dumps a chemical called CGRP into both your cranial blood vessels and your scalp tissue. This chemical causes intense inflammation in the skin of your scalp, making normal actions like brushing your hair or tying a hijab incredibly painful.
Q: Is "tension headache" just another word for migraine? A: No, though they often overlap. Tension headaches are primarily driven by mechanical, muscular contraction—often a tight "band" of pressure wrapping around the forehead and the base of the skull directly caused by staring at KL office screens or poor commuter posture. Migraines are a severe neurovascular event involving entirely different pain pathways and often include nausea and light sensitivity.
Q: How often should I get a head spa if I suffer from chronic tension headaches? A: To effectively manage chronic muscular tension and maintain high vagal tone (parasympathetic relaxation), a bi-weekly session is optimal during a severe flare-up, moving to a monthly maintenance cadence once the frequency of the headaches has subsided. Consistent preventative care is far more effective than trying to treat a migraine once it has already fully developed.
***
References
- Edvinsson, L. (2017). *The Trigeminovascular Pathway: Role of CGRP and CGRP Receptors in Migraine*. Headache: The Journal of Head and Face Pain, 57(S2), 47-55.
- Straube, A., Ellrich, J., Eren, O., Blum, B., & Ruscheweyh, R. (2015). *Treatment of chronic migraine with transcutaneous stimulation of the auricular branch of the vagal nerve (auricular t-VNS): a randomized, monocentric clinical trial*. The Journal of Headache and Pain, 16(1), 543.
- Goadsby, P. J., Holland, P. R., Martins-Oliveira, M., Hoffmann, J., Schankin, C., & Akerman, S. (2017). *Pathophysiology of Migraine: A Disorder of Sensory Processing*. Physiological Reviews, 97(2), 553-622.
- The Migraine Trust. (2020). *State of the Migraine Nation*. Reporting on global prevalence and the economic impact of migraine.
